Betty Lou, finally having completely recovered from the latest foot operation, suddenly began experiencing pain in her left thumb, in two places. Often, just moving the thumb caused excruciating pain at the joint at the base of the thumb, and flexing the joint above it was also a problem. First the bone would not move, then, with increasingly applied pressure, it would suddenly, painfully, pop into position. As is usual in today's medical system, it took her quite a while to be able to progress to the point where she was able to consult with an expert who could determine what the problem was.
As the symptoms suggested, the causes were twofold:
• Osteoarthritis at the base of the thumb metacarpal had worn through the cartilage between it and the bone against which it pivoted, the trapezium, and in fact had eroded most of that bone.
• Tendon inflammation had caused "trigger thumb;" as you may guess, a relative of trigger finger. A nodule on the tendon makes it difficult for it to slide through ligament sheaths ("pulleys") adjacent to the metacarpal joints. The nodule resists tendon movement until sufficient force is applied, when it will suddenly, painfully, pop through.
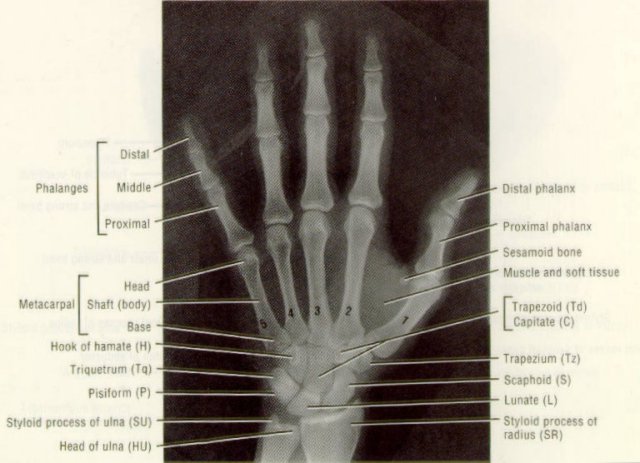
This picture shows the relation of the trapezium to the thumb metacarpal and the normal positions of the thumb phalanges, also called phalanxes.
This is an x-ray of Betty Lou's left hand taken in 1985; normal at that time.

This x-ray reveals the recent damage. The circle highlights the affected area – most of the trapezium seems to have turned into sand. And the line shows how far the proximal phalange sometimes could move out of a normal position.

Both conditions required surgery.
It turns out that hand surgery is an exacting specialty. The myriad motions that can be performed by the fingers, not to mention our unique opposable thumbs, require an extensive network of bones, joints, tendons, ligaments, blood vessels, and nerves. Medical researchers have developed a representation of the human nervous system that graphically illustrates this complexity. Called a homunculus, it is a diagram of a "little person," the size of whose features are proportional to the number of nerve endings they require in the brain.

Although Betty Lou also consulted a hand surgeon at the Curtis Hand Institute in Baltimore and a surgeon at Georgetown Hospital, her research showed that Dr. Lovallo, originally recommended by her primary care physician, was highly respected in the field. By coincidence, one evening when she met a woman at a gallery opening who had had the same operation a year before and was completely satisfied with the result, she found that her doctor had studied under Dr. Lovallo.
The thumb arthritis repair would involve removal of the remnants of the trapezium, to be replaced by a pad formed by a spare tendon removed from the lower arm. Who knew we had spare tendons for such useful purposes?
To repair a trigger thumb, the tendon is "released" by slicing the appropriate sheath. However, in Betty Lou's case, a ligament, the volar plate,
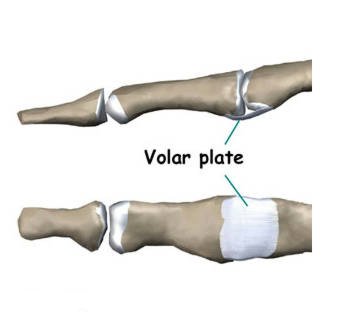
also required repair. This ligament, on the palm side of the thumb, holds the joints together and prevents the thumb from "hyperextending" – moving too far outward. As the recent x-ray shows, this ligament had ceased to do its job. Although this can be caused by stretching of the ligament, it turned out that it was actually torn, requiring installation of an "anchor" into the bone, to which the torn ligament could be stitched.
The late-September hospital experience again turned out to be a disaster (i.e., see Hardware). Told to arrive at 9 AM for an 11 o'clock operation, she wasn't even taken in to the preparation area until 3 PM. The anesthesiologist introduced himself and described what would be occurring. He was an interesting person; in his 30's, he said he enjoyed golfing. We asked how good a golfer he was. It turned out he was good enough to play on the PGA tour for a year, but not good enough to make a decent living at it, so he returned to anesthesiology! He also had had a heart attack several years earlier, and was currently running more weekly miles than I.
However, these preliminaries turned out to be wasted, because he went off duty before her turn came and she never met the actual anesthesiologist before she was wheeled in to the operating room. She had been told that after the operation, the anesthesiologist would talk to her before she left; she was left in a waiting area for hours but he never appeared. She was requested to sign a release form that didn't have her name on it! We finally were able to leave, after twelve hours, her sling bloody. On our departure, we were given a prescription for pain medication, which she definitely needed by then. Why it couldn't have been presented sometime earlier during the entire day I sat there waiting, so I could have it filled by then, is another mystery.
The thumb was held in position internally by a pin which projected outside the side of the thumb, and externally by a splint and many wrappings.

A week later LaTonya removed the wrappings (the picture shows the pin and one of the incisions required to remove the trapezium and insert the spare tendon)

and applied a blue cast

which she removed a month later

This picture shows the incisions on the forearm where the "spare" tendon was removed [circled], the incisions required to repair the trigger thumb, and the pin

which Dr. Lovallo extracted. In spite of what it looks like, it wasn't painful -- it was the anticipation!

For this operation there had been no necessity for an x-ray while the pin was in place. One taken later shows the gap left by the trapezium bone's removal, the spare tendon now filling the gap being invisible to x-rays. The anchor for the volar ligament can be seen at the upper right.

Since then Betty Lou has gone to physical therapy twice a week, and done "homework" three times a day. It's quite time-consuming, requiring first applying moist heat to the area with a "hydrocollator" pad. She then manually massages the thumb and adjacent fingers to decrease edema and reduce scar tissue, manipulates the joints, uses a pressure ball and a mechanical massager on the tendons, and weight exercises to restore flexibility – after six weeks of immobility, she couldn't move her thumb or wrist.
She has found, similarly to her experiences after her foot surgeries, that many others don't bother doing their homework and complain about their lack of progress. Her physical therapist has presented Betty Lou to them as her poster patient.
Throughout, the pain has been much more severe than after her foot operations – evidently the homunculus is accurate. It seems that complete recovery from this latest operation may also take a year. Meanwhile, her right foot is starting to exhibit symptoms similar to those that required the left-foot bunionectomy.